
In the recently published ‘3D bioprinting and its potential impact on cardiac failure treatment: An industry perspective,’ authors Ravi K. Birla and Stuart K. Williams explore the potential for tissue engineering in cardiac medicine, and the eventual assembly of a bioprinted heart.
While heart failure usually requires a transplant, it can be challenging to find a suitable donor. Once a transplant is completed, there is a long road ahead too via a permanent need for immune suppression therapy—treatment that is hard on patients. The usual survival rate for patients is typically under 13 years.
“There are currently more than 6.2 million patients in the US with heart failure, and heart failure accounted for 78,356 mortalities in 2016,” stated the authors.
In this study, the researchers review the challenges of bioprinting for the creation of heart tissue, as well as the ‘logical and systematic process to bioprint human heart.’
While medical science is full of progressive tools, treatments, and devices—especially for heart patients—no technology has been more promising for the eventual fabrication of organs than tissue engineering. With the potential to yield a biofabricated heart, made up of both ‘biologic and artificial construct,’ a total heart could feasibly emerge with modular parts for easy replacing.
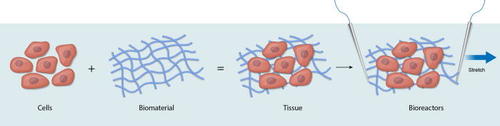
Definition of tissue engineering—the building blocks of tissue engineering are cells, biomaterials, and bioreactors. Cells are the functional elements of all tissue and organs, while biomaterials are designed to simulate the mammalian extracellular matrix and provide structural support. Bioreactors are custom devices to deliver physiological cues for 3D tissue/organ development and maturation. Electrical stimulation is delivered by parallel electrodes, while uniaxial stretch, illustrated by the single arrow, is designed to apply cyclic movement of the bioengineered tissue.
Cardiac tissue engineering encompasses:
- 3D printed cardiac patches
- Biological pumps
- Ventricles
- Valves
- Blood vessels
- Comprehensive bioartificial hearts
“The ability to bioengineer components of the heart or the entire bioartificial heart, both have applications in changing the standard of care for patients with heart disorders,” explained the authors. “Depending on the severity of the patient, a cardiac patch may be sufficient to augment lost contractile function, while in cases of chronic heart failure, a total bioartificial heart may be required.”
“In addition to spatial regulation of the cells, bioprinting also allows accurate placement of the biomaterials. This is where 3D bioprinting provides a powerful tool that allows us to accurately position different cell types in a very specific pattern, thereby allowing tight control over the heart bioengineering process.”
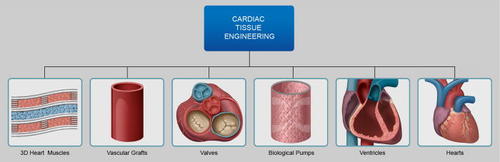
Overview of cardiac tissue engineering—the field of cardiac tissue engineering includes methods to bioengineer contractile 3D heart muscle, biological pulsating pumps, bioengineered left ventricles, bioartificial valves and vascular grafts, and biofabricated hearts. Contractile 3D heart muscle is designed to replicate the properties of mammalian heart muscle tissue and can be used as a patch to augment left ventricle pressure after myocardial infarction. Pulsating pumps are designed to generate intra-luminal pressure and can be used as biological pumps. Left ventricles can be used as a component of the heart or to replace under-performing ventricles in pediatric cases of hypoplastic left heart syndrome. Valves and vascular grafts can be used to replaced mammalian valves and blood vessels or as components of the bioengineered heart.
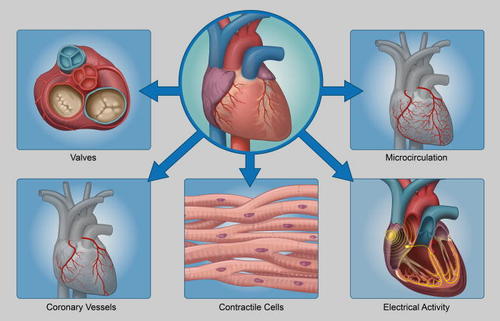
Major components of the human heart—the human heart consists of four chambers, four valves, the cardiac conduction system, contractile cardiomyocytes, and a complex vasculature. The four chambers are the left and right ventricle and aorta, while the four valves are the aortic and mitral valves and pulmonary and tricuspid valves. The cardiac conduction system consists of the SAN, AVN, bundle of His, and the Purkinje fibers. Cardiac vasculature consists of the greater vessels as well as the smaller micro-circulation. Cardiomyocytes are the cells responsible for heart muscle contraction.
So far, most research involving bioprinting of cardiac tissue has shown the ‘initial feasibility of bioprinting hearts.’ With the amount of research and tools available today, such progress is inevitable.

“Based on the current state of the art in whole heart bioengineering, we can safely say that human hearts will be available for clinical transplantation though we cannot assign a specific timeframe for this fate to be accomplished,” state the authors.
Bioprinting of the human heart has its beginnings in the initial history of tissue engineering in 2003, and then further in research a few years later.
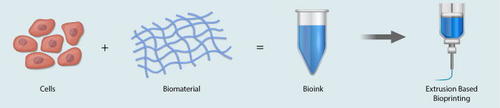
The 3D bioprinting process—isolated cells are suspended in a custom formulated bioink and loaded into a syringe. Examples of cells required to bioprint hearts include contractile cardiomyocytes, conducting pacemaker and Purkinje cells, structural fibroblast cells and vascular smooth muscle cells, and endothelial cells. Pneumatic pressure is used to extrude the cell-loaded bioink through the printing tip, and a layer by layer approach is used to build tissue and/or organ

Scientific breakthroughs for 3D bioprinting human hearts.
There has continued to be rapidly growing success in bioprinting and the subsequent fabrication of heart tissue, allowing scientists to realize less of fantasy in such exercises—and more of a reality.
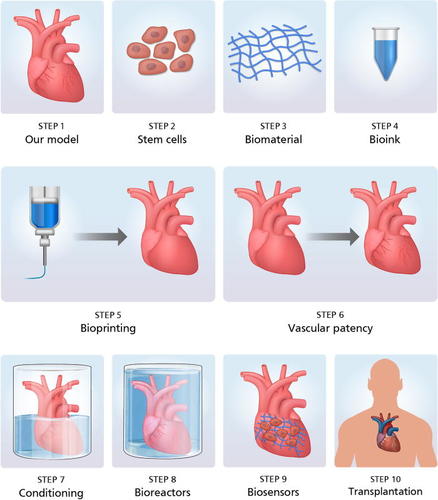
Process for bioprinting human hearts—patient MRI images are used to model the heart. Dermal fibroblasts are isolated from patient skin biopsies and converted to iPS cells and then to cardiomyocytes. Cardiomyocytes are combined with bioinks and used to bioprint patient-specific human hearts. Bioprinted hearts are conditioned in bioreactors and used for transplantation.
The roadmap for bioprinting a heart includes:
- 3D printing of the microcirculation
- Construction of coronary macrovascular structures
- 3D bioprinting for the cardiac conduction system
- 3D bioprinting for heart valves
- 3D bioprinting for cardiac muscle
“The single most important challenge that needs to be overcome in the field, and one that in general staggers the field of cardiac stem cell therapy, is the immaturity of reprogrammed cardiomyocytes,” conclude the researchers. “Conversion of iPS cells to cardiomyocytes is now standard and reproducible, the differentiated cells resemble an embryonic phenotype, and driving these cells to an adult phenotype remains a critical challenge in the field of cardiac stem cell therapy.”
“Once reproduced by independent research labs, coupled with the availability of commercial bioreactors for electromechanical stimulation, the availability of mature cardiomyocytes will provide a clear pathway to 3D bioprint human hearts for clinical transplantation.”
Bioprinting is used in a wide variety of applications today, from cardiac patches and cellularized hearts to the creation of heart valves, and more, ultimately shaping an overall transformation of cell culture. What do you think of this news? Let us know your thoughts! Join the discussion of this and other 3D printing topics at 3DPrintBoard.com.
[Source / Images: ‘3D bioprinting and its potential impact on cardiac failure treatment: An industry perspective’]
The post The Progress & Ongoing Challenge of 3D Bioprinting Cardiac Tissue appeared first on 3DPrint.com | The Voice of 3D Printing / Additive Manufacturing.