Lars Brouwers is a surgeon in training and a researcher at the Radboudumc and the Elisabeth-Tweesteden hospital. He investigates the value of 3D printing and Virtual Reality in the treatment of complex fractures. With his research he received the AOTrauma Europe Research Grant and has won the Technical Innovation Award from the European Society for Surgical Research (ESSR), the international award of the Orthopedic Trauma Association (OTA), the Canadian and American sister association of the Dutch Nederlandse Vereniging voor Traumachirurgie (NVT) and the national IT award for “best IT project in healthcare” (Computable awards). In December 2017 he drove with an old car to Sierra Leone, equipped with a 3D printer (Ultimaker 2+), to develop a sustainable way in improving prosthetic arms and legs for handicapped people and making spare parts for a hospital there. One-and-a-half years later, a medical 3D printed lab is up and running in the Masanga Hospital. Now for the second time, a technical medicine student from the Netherlands is investigating 3D printed prostheses there. For this work, he received the Dutch Albert Schweitzer fund (NASF) grant. Lars is a really inspirational person really making more happen with 3D printing in medicine so we decided to interview him.

Who are you?
I’m Lars Brouwers, live in a small town near ‘s-Hertogenbosch in the southern part of the Netherlands, 30 years old and work in two major trauma centers (Elisabeth-Tweesteden Hospital, Tilburg and Radboudumc, Nijmegen) as a surgeon in training.
What do you hope to achieve?
Besides being trained to be a surgeon in two top-clinical healthcare centers, I investigate the role of 3D printing in the medical world. I believe 3D printing is the next important invention after the internet. With 3D printing, we could provide patients, residents, nurses and physicians the best medical care there is.
How do you use 3D printing?
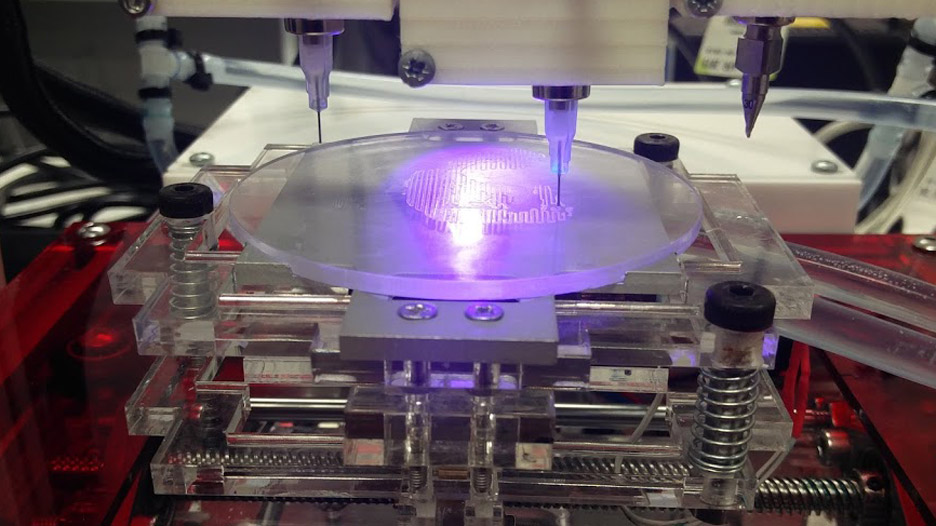
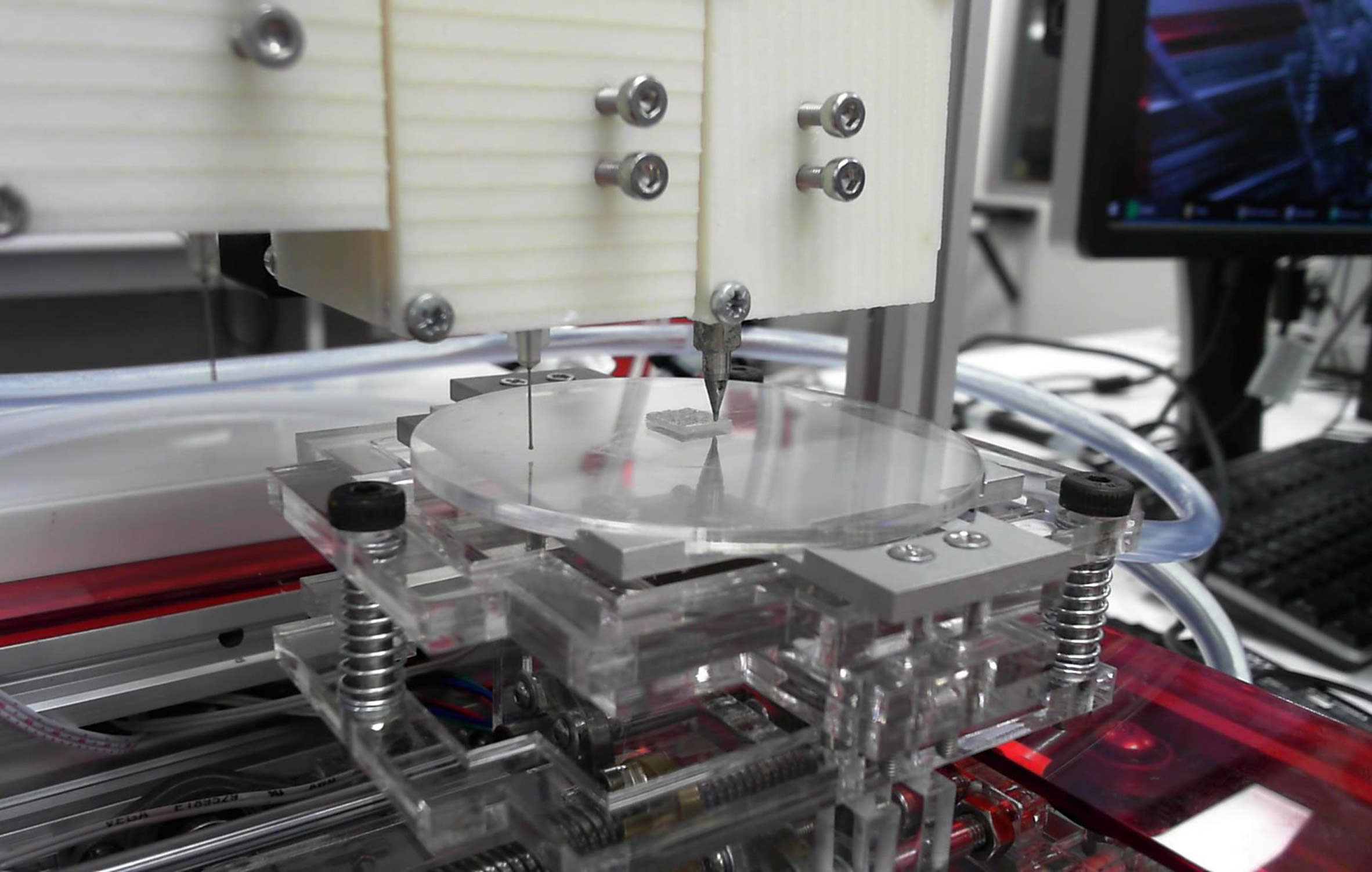
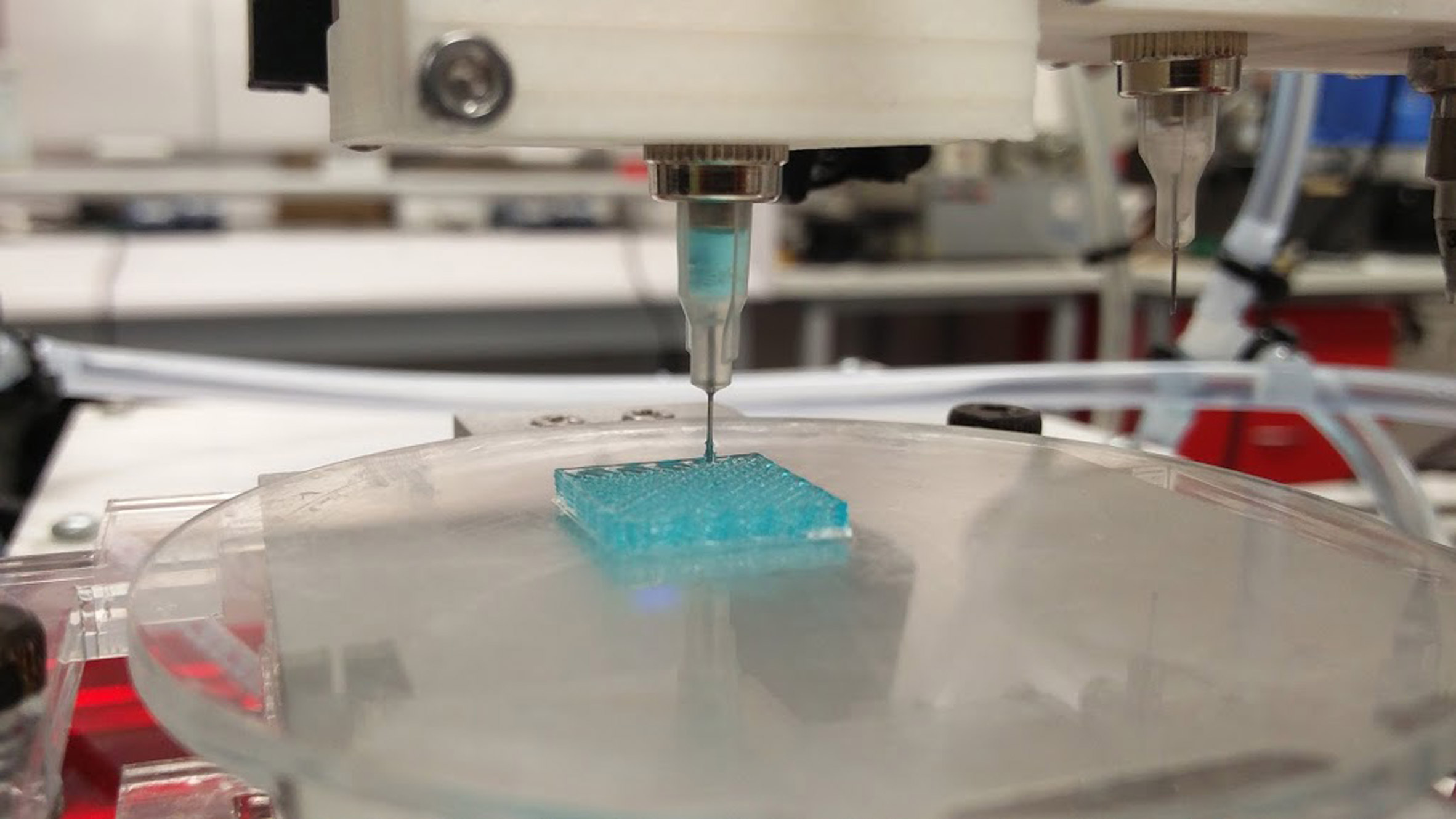
We use 3D printing for building life-size anatomical models and molds for surgical procedures. We set up several in-hospital medical 3D labs to ensure a 24/7 workflow without the need for technicians. 3D printing for doctors, by doctors. Low costs, and with the use of easy to use software systems.
How does it help doctors and what research do you need to do in order to use more 3D printing in your work?
Dr. Mike Bemelman, traumasurgeon, Dr. Jan Heyligers, vascular surgeon and I set up our medical 3D lab in 2016 in the Elisabeth-Tweesteden hospital. We have expanded our 3D lab to a fully up and running 3D print lab in which we can 3D print anatomical models for surgeons, residents, nurses and patients 24/7. Our 3D print lab is now an example in the Netherlands of how a non-profit lab could and should work.
We think 3D printing, is the next invention after Xray and CT. Using 3D printed models, surgeons are able to expand their surgical preparations. 3D printed models provide a 3D view, while using conventional diagnostics brains are needed to form “virtual 3D models” in the head of the surgeon. Some people say, 3DCT is another solution. However, last year we demonstrated the added value of 3D printing in classifying complex fractures fractures (Brouwers, Lars, et al. “The Value of 3D Printed Models in Understanding Acetabular Fractures.” 3D Printing and Additive Manufacturing 5.1 (2018): 37-46.). Furthermore, we have showed for the first time that a 3D printed model is exactly the same as a human cadaver (Brouwers, Lars, et al. “Validation study of 3D-printed anatomical models using 2 PLA printers for preoperative planning in trauma surgery, a human cadaver study.” European Journal of Trauma and Emergency Surgery (2018): 1-8.)
At this moment we are investigating the role of 3D printing in explaining fractures and aneurysms to patients. Is it possible that patients are more satisfied or have a better understanding of their injury when 3D printed models of their own body are using during the explanation.
The 3D printing industry sometimes sees 3D printing as the holy grail. However, we have to be critical. If you treated one case with a 3D printed model and you are satisfied with the result, is it because of the 3D printed model or something else? The supposed advantages of 3D printing can only be proven by doing a lot of research. Some people say, that because of 3D printing, the operation time is shorter. However, is 10 minutes shorter really important? And they say that less blood loss occurs and operations will get cheaper. However, the preoperative workup gets more expensive. So, in what way is it really true that 3D printing is cost-effective?! A lot of research is needed and not case reports about how fantastic 3D printing is, based on 1 or 3 cases.
For what kind of cases do you use it?
 We use 3D printing mainly for traumasurgery cases. Patients with broken bones due to a fall, car accident or shooting, stabbing. We also 3D print aneurysms of the aorta to visualize the abdominal aneurysms for the patients preoperatively and postoperatively. At the moment we are testing with 3D printing soft tissue, such as esophagus cancer or anal fistulas. However, this is much more complex because the density of the tissue looks more like the surrounding tissue. An automatic threshold is in these cases not possible and we have to extract all the specific tissue by hand.
We use 3D printing mainly for traumasurgery cases. Patients with broken bones due to a fall, car accident or shooting, stabbing. We also 3D print aneurysms of the aorta to visualize the abdominal aneurysms for the patients preoperatively and postoperatively. At the moment we are testing with 3D printing soft tissue, such as esophagus cancer or anal fistulas. However, this is much more complex because the density of the tissue looks more like the surrounding tissue. An automatic threshold is in these cases not possible and we have to extract all the specific tissue by hand.
What printers and materials do you use?
We use several 3D printers. In Sierra Leone an Ultimaker 2, in Tilburg an Ultimaker 3+, Makerbot Replicator Z18 and a Formlabs 2 and in Nijmegen two Ultimaker S5’s. We print with PLA, PVA and TPU 95A.
How is 3D printing limited for you?
I do not see any limited subject regarding 3D printing at the moment. How I see it, is that we are working with an ”iPhone 1.0”. The technique is here, however, it can get faster and better. But we are satisfied with what we have accomplished so far.
What partnerships do you seek?
We cooperate with both 3D printing companies such as Ultimaker and other hospitals to gain more knowledge about medical 3D printing. We have helped set up non-profit low-budget medical 3D labs in the Hospitals of Assen, Enschede, Nijmegen, Roosendaal and Rotterdam. Every hospital has his own radiology department with their own software. So converting CT files (DICOM) into STL files is in every hospital different. Some hospitals have own 3D software (Philips, Siemens) and other buy 3D software from 3D software companies (Mimics for example.). Therefore, we are cooperating with the largest medical 3D lab of Europe: 3D lab Radboudumc, head of department is Prof. dr. Thomas Maal. They are investing the role of artificial intelligence on the operation room and the role of augmented reality. Furthermore, his team takes care of several preoperative evaluations for all kinds of operations using molds and guides. Together we are investigating non-profit 3D software in order to set up 3D labs worldwide.
Last, we cooperate with the technical University of Twente. Technical medicine students are the connection between doctors and medical technique and are becoming more and more important. Together with their students, we can expand our 3D labs and ensure a proper 3D understanding for doctors and patients. For example, if we have a case with a malunion of the wrist, a technical medical engineer and treating physician are sitting together to prepare the operation and design guides or molds in order to correct the malunion in the best way there is. The engineer is also present during the operation. So they think, act and discuss together. A new way in improving patient outcomes!
Why Sierra Leone?
A friend of mine, Wouter Nolet, is working as a doctor in the Masanga hospital, in the heart of Sierra Leone. Furthermore, he runs the Capacare programma in which local physicians are being trained in order to perform the most common surgical procedures. After graduation, they will work in several small remote hospitals of the country. A beautiful sustainable project! Together we decided to drive to Sierra Leone using his old Swedish car, a Saab 9.5 Turbo from the year 2001. I already thought for a while about the idea of implementing 3D printing in third world countries. This was an excellent opportunity to investigate the role of 3D printing in a local hospital. We put an Ultimaker 2+ in de back of the car and drove in 3 weeks time from the Netherlands, through Belgium, France, Spain, Morocco, Mauritania, Senegal, Guinea to Sierra Leone.

What have you accomplished there?
In cooperation with the 3D lab of the Radboudumc, we set up a backup team for soft- and hardware problems. On-site we discussed with local people and tropical doctors to check the need of 3D printing. Based on this fieldwork, we found out that 3D printing could be of importance for making prostheses, spare parts and anatomical models for physicians. Many patients were living in camps nearby and we found out that the conventional prostheses were expensive to make. First we tried to help a woman with a burned hand. She wanted to write again. We took photos, used whatsapp to send the photo’s to the 3D lab in the Netherlands, designed a functional prosthesis and 3D printed this in the hospital. Due to this, she could write again!

Furthermore, the umbilical cord clamps appeared to be finished in the hospital, so we 3D printed them as well. However, we were not satisfied with the workflow and added the head of the department of Utwente, Prof. Slump and prof. Grobusch, professor of tropical medicine, of the University of Amsterdam. Together with Jonathan Vas Nunes, the tropical Doctor, and director of the Masanga Hospital and Arico Verhulst, medical technician, we improved our concept and send for the first time a Technical medicine student, Merel van der Stelt, for 3 months to Sierra Leone, to investigate the role of 3D printing. She soon found out that patients found it more important to wear aesthetic prostheses when compared with functional prostheses. She used a 3D handscanner to scan the contralateral arm and mirrored this model. We are now able to 3D print prosthestic arms in less than 24 hours. Merel is investigating the lower extremity 3D printed prosthesis at the moment (even more challenging!) and a new technical medicine student, Andrea Sterkenburg, will soon fly to Sierra Leone to test different 3D printed prosthesis and investigate the sustainability. We continue with the follow-up of our patients to investigate the short-term and long-term quality of life and satisfaction about the prostheses. So far, it looks like that patients are satisfied about the strength and design. Even though the prostheses were aesthetic, they also seem to exhibit some degree of functionality. Even more important, ethical approval for this study has been obtained by the Sierra Leone Ethics and Scientific Review committee.

What advice do you have for people who wish to help developing countries with 3D printing?
Helping people in third world countries is all about sustainability. With all respect to the many international teams who are going to African countries to help for 2-3 weeks, “giving” people prostheses for free is not sustainable. If you give local people everything for free, they do not understand that is normal to pay for a product, although it is a small amount of money. I will give you an example. In Africa, several hospitals are being run by local doctors. Local people have to pay a small amount of money for being treated, like in the western world. Only in this way, employees can be paid and the hospital can survive of course. It is not sustainable to live and survive on grants from western countries. However, every now and then a small (surgical) team from a western country arrives and announces that they treat as many as people they can treat in 2-3 weeks for free. Besides the lack of aftercare, it is confusing for local people when to pay or not? And people then refuse to pay the local doctors for treatment after this period. Therefore, our concept is to build a sustainable 3D workplace, in cooperation with local prostheses shops and in cooperation with local hospitals. We examine at the moment, how much local people can afford to pay for a 3D printed prosthesis and are making contracts with local shops in order to get sustainable.
What advice do you have for physicians who wish to use 3D printing more?
Trial and error! Innovations and failing are related to each other. If there is no failing, anyone can innovate. Therefore it is important to keep on trying an believe in your own ideas! Be critical and do research in order to prove 3D printing is the technique of the future. Proper understanding and research is needed to draw conclusions!





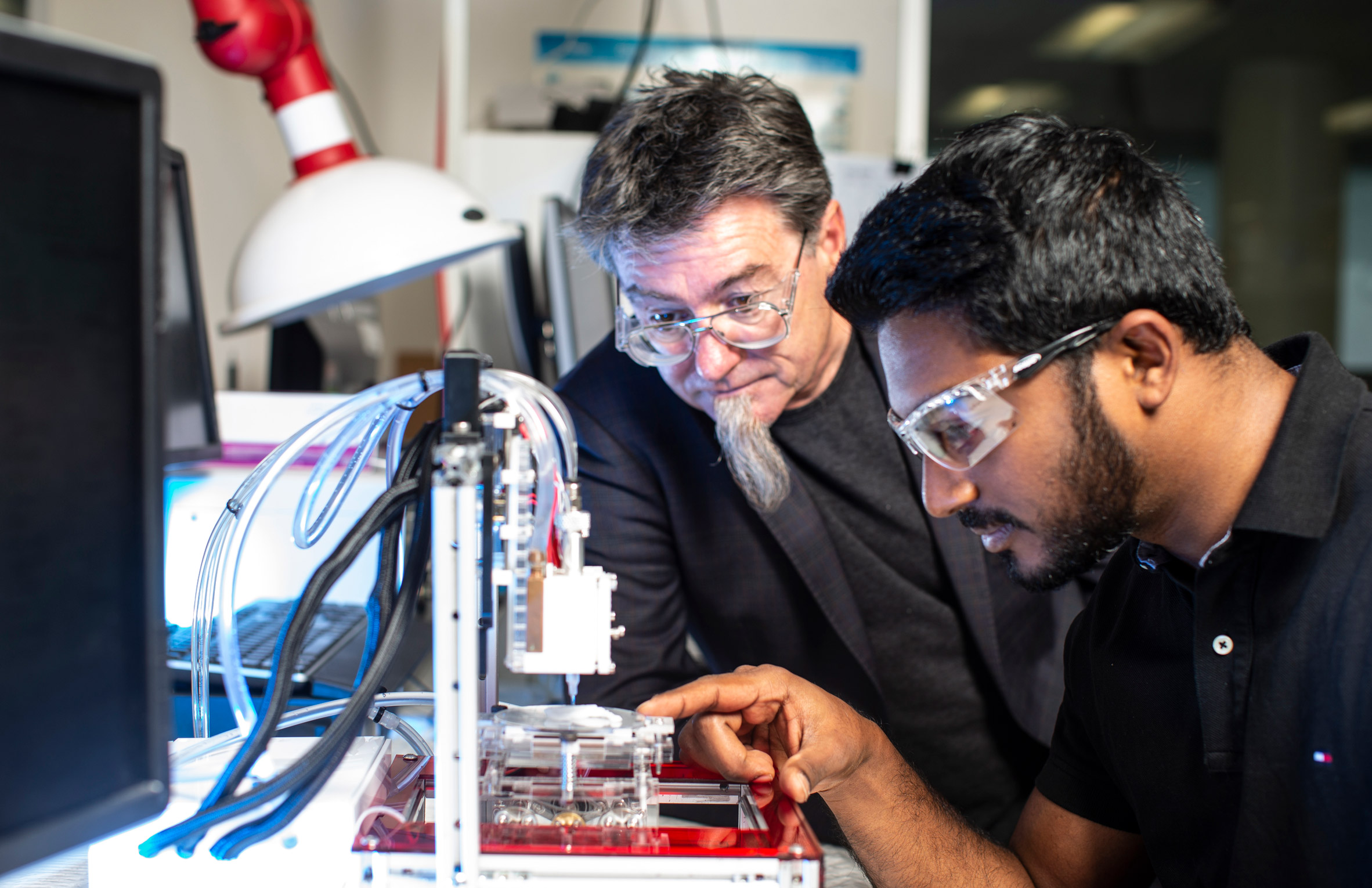 Image via Dezeen
Image via Dezeen