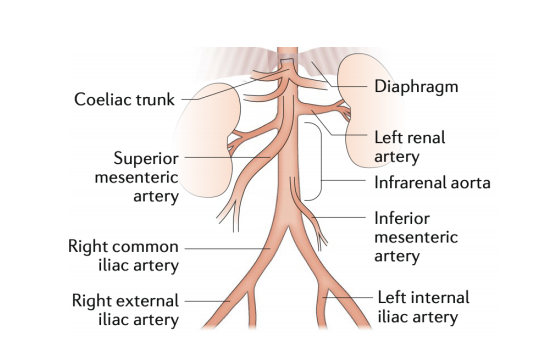
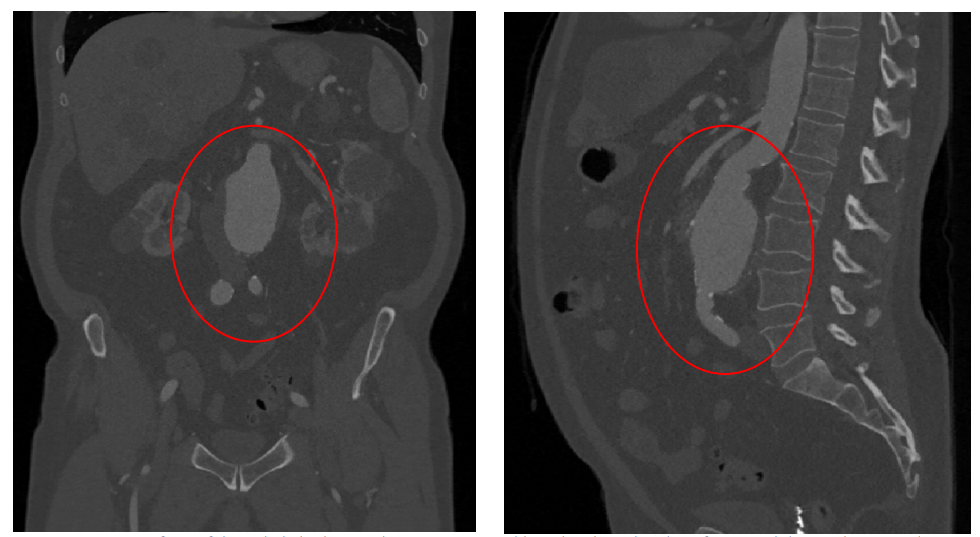
Peripheral Arterial Disease (PAD) is a condition which sees fatty deposits collect and lower the blood flow in arteries outside of the heart, most commonly in the legs. Those suffering from PAD will often experience pain while walking, and could even develop gangrene if the case is serious enough. Over 10 percent of people in Australia are afflicted with this painful condition. To treat it, a stent can be temporarily inserted inside the blood vessel to keep it open.
![]() We’ve seen 3D printing used to fabricate stents before, which can help improve sizing options and allow for patient-specific diameters and shapes. But ,until now, there hasn’t been a way to print a self-expandable stent made of shape-memory nickel and titanium alloy nitinol. The material is superelastic, and metallurgists have had a difficult time trying to figure out a way to 3D print a self-expandable nitinol stent without compromising the unique properties of the metal alloy.
We’ve seen 3D printing used to fabricate stents before, which can help improve sizing options and allow for patient-specific diameters and shapes. But ,until now, there hasn’t been a way to print a self-expandable stent made of shape-memory nickel and titanium alloy nitinol. The material is superelastic, and metallurgists have had a difficult time trying to figure out a way to 3D print a self-expandable nitinol stent without compromising the unique properties of the metal alloy.
But researchers from Australia’s national science agency, the Commonwealth Scientific and Industrial Research Organisation (CSIRO), together with its Wollongong-based partner, the Medical Innovation Hub, have finally made it possible.
Vascular surgeon Dr. Arthur Stanton, the Chief Executive of Medical Innovation Hub, explained, “Currently, surgeons use off-the-shelf stents, and although they come in various shapes and sizes, overall there are limitations to the range of stents available. We believe our new 3D-printed self-expanding nitinol stents offer an improved patient experience through better fitting devices, better conformity to blood vessel and improved recovery times. There is also the opportunity for the technology to be used for mass production of stents, potentially at lower cost.”

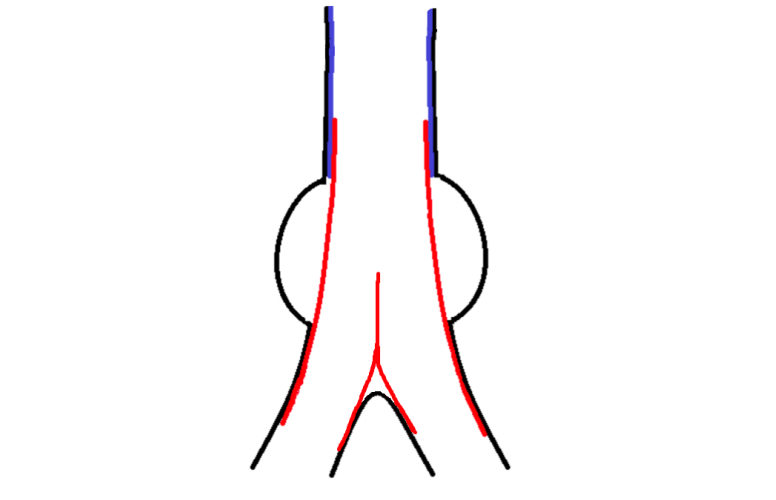
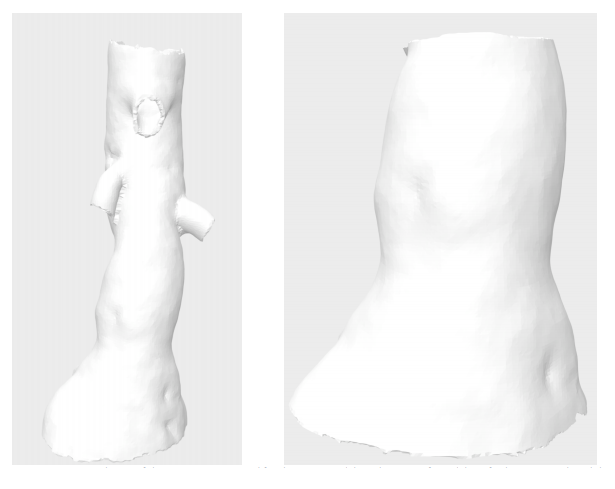
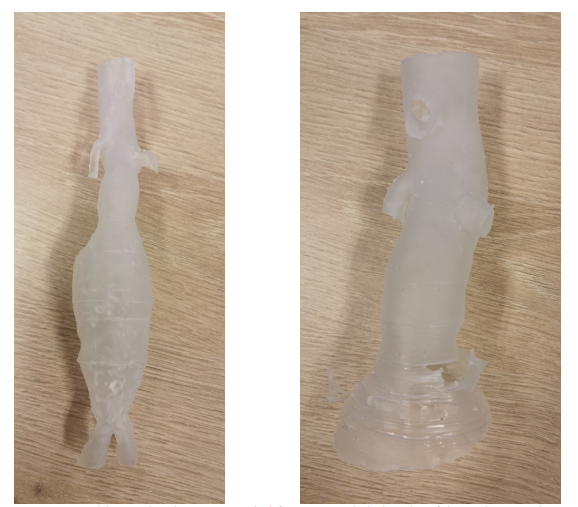
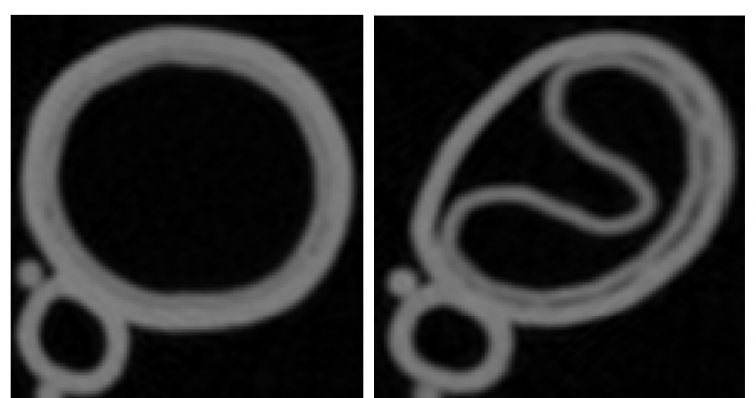
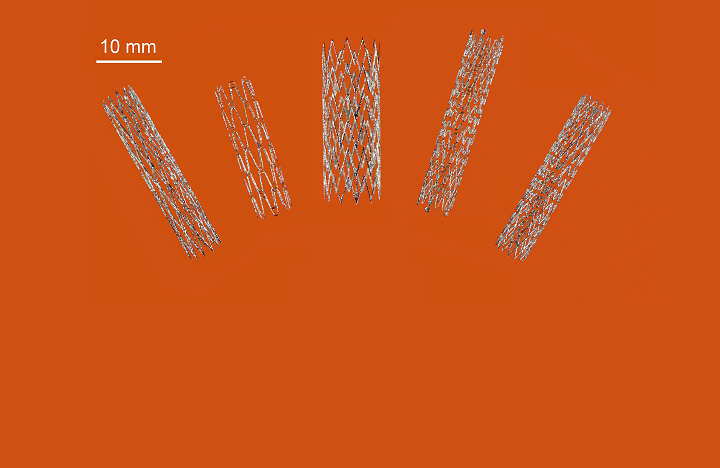
Stent model
The first 3D-printed nitinol stent is a major medical breakthrough for PAD patients, as surgeons have had to use off-the-shelf, non-custom stents for these procedures in the past. But with 3D printing, individual nitinol stents can be made right at the hospital, with the surgeon there to offer instructions—saving time and money, and reducing inventory, as well.
According to Australia’s Minister for Industry, Science and Technology, Karen Andrews, 3D printing could mark a major paradigm shift in the $16 billion worldwide stent manufacturing industry:
“This is a great example of industry working with our researchers to develop an innovative product that addresses a global need and builds on our sovereign capability.”
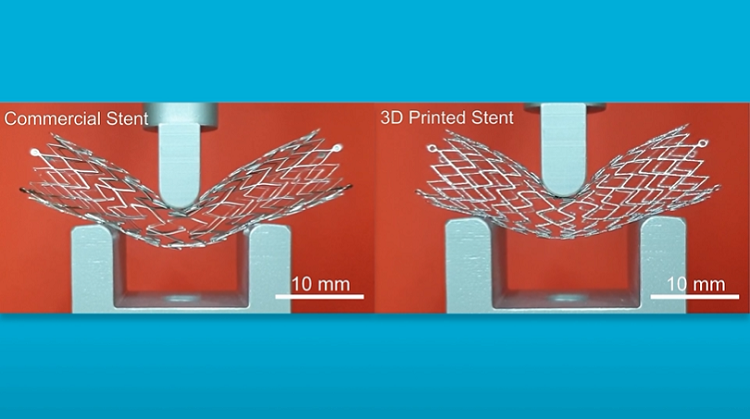
The proof-of-concept stents offer the potential for customization to individual patient requirements, but are equally as suitable for mass production.
Back in 2015, CSIRO opened the Lab22 Innovation Center. The specialist researchers there are focused on creating value for Australia’s manufacturing industry by developing future developments in metal additive manufacturing. CSIRO’s Lab22 collaborates with industry partners, like the Medical Innovation Hub, to build important biomedical parts, like the first 3D-printed sternum and titanium heel, and now the first 3D-printed nitinol stent.
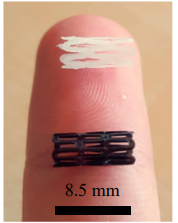
CSIRO Principal Research Scientist Dr Sri Lathabai said, “Nitinol is a shape-memory alloy with superelastic properties. It’s a tricky alloy to work with in 3D printing conditions, due to its sensitivity to stress and heat. We had to select the right 3D-printing parameters to get the ultra-fine mesh structure needed for an endovascular stent, as well as carefully manage heat treatments so the finished product can expand as needed, once inside the body.”
The team used selective laser melting (SLM) technology to successfully fabricate the complex mesh stent structures. Due to the level of geometric accuracy that 3D printing achieves, the stents can be made for specific patients, and nitinol allows them to expand once inside the body. CSIRO has established a new technology company, Flex Memory Ventures (FMV), to help commercialize the technology.
Discuss this story and other 3D printing topics at 3DPrintBoard.com or share your thoughts in the Facebook comments below.
The post CSIRO 3D Prints First Self-Expandable Stents from Shape-Memory Alloy Nitinol appeared first on 3DPrint.com | The Voice of 3D Printing / Additive Manufacturing.